























Reserve Bank of India (RBI) has setup Supervisory Colleges for the six Scheduled Commercial Banks with sizeable international presence. They are State Bank of India, ICICI Bank Ltd., Bank of India, Bank of Baroda, Axis Bank Ltd. and Punjab National Bank.
The objectives of the colleges are to enhance information exchange and cooperation among supervisors, to improve understanding of the risk profile of the banking group and thereby facilitate more effective supervision of internationally active banks.
This was stated by Santosh Kumar Gangwar, Minister of State for Finance in written reply to a question in Lok Sabha on July 28.
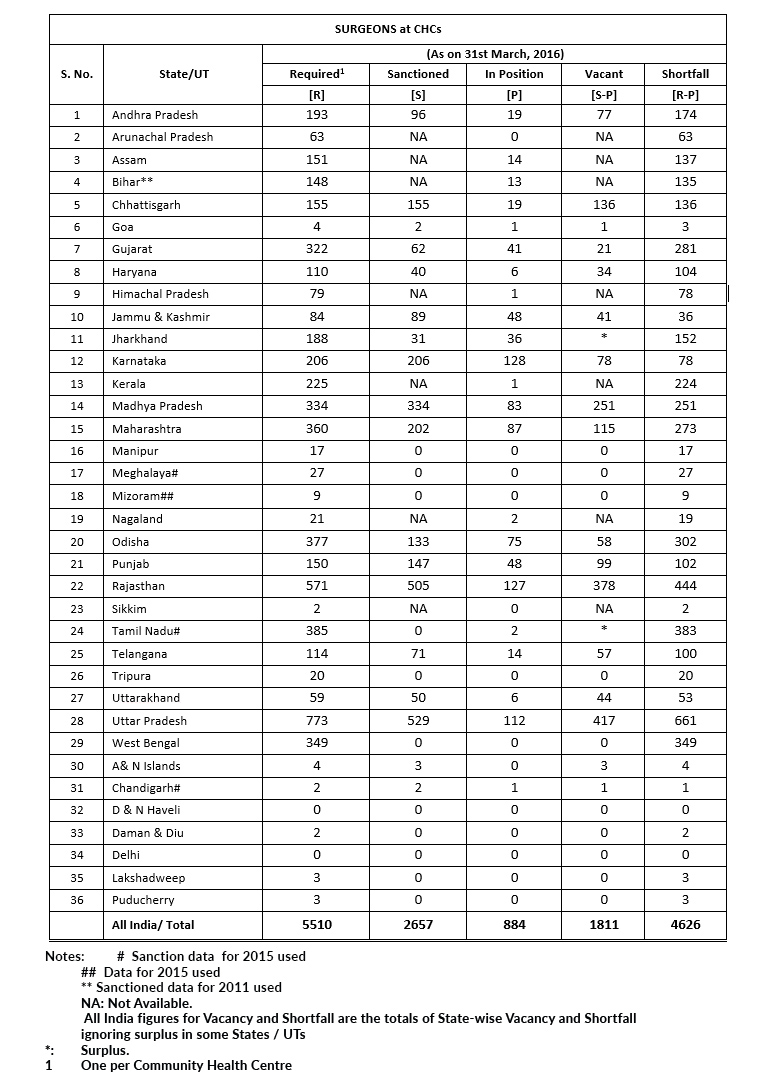
Healthcare Infrastructure
As per Rural Health Statistics (RHS) 2016, there is shortage of specialist doctors in Community Health Centres (CHCs). State/UT-wise status of availability of specialist doctors including surgeons, physicians, pediatricians and gynecologists is given below:
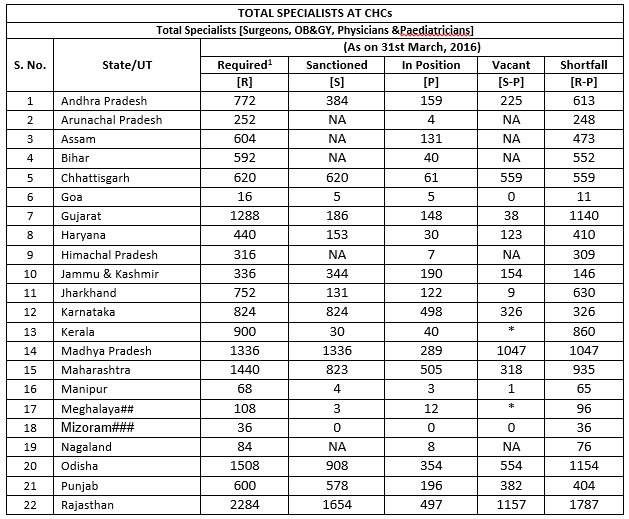

Public health and hospitals being a State subject, the primary responsibility to ensure availability of specialist doctors in public health facilities lies with the State/UT Governments. However, under the National Health Mission (NHM), financial and technical support is provided to States/UTs to strengthen their healthcare systems including support for insourcing or engagement of specialist doctors on contractual basis, based on the requirements posed by the States/UTs in their Programme Implementation Plans (PIPs) within their overall resource envelope.
Support is also provided to States/UTs for hard area allowance to specialist doctors for serving in rural and remote areas and for their residential quarters so that they find it attractive to serve in public health facilities in such areas.
The Government has taken various steps to improve the overall availability of doctors and Specialists in the country. These steps include:
- The ratio of teachers to students has been revised from 1:1 to 1:2 for all MD/MS disciplines and 1:1 to 1:3 in subjects of Anaesthesiology, Forensic Medicine, Radiotherapy, Medical Oncology, Surgical Oncology and Psychiatry in all medical colleges across the country. Further, teacher: student ratio in public funded Government Medical Colleges for Professor has been increased from 1:2 to 1:3 in all clinical subjects and for Associate Prof. from 1:1 to 1:2 if the Associate Prof. is a unit head. This would result in increase in number of specialists in the country.
- DNB qualification has been recognized for appointment as faculty to take care of shortage of faculty.
- Enhancement of maximum intake capacity at MBBS level from 150 to 250.
- Enhancement of age limit for appointment/ extension/ re-employment against posts of teachers/dean/principal/ director in medical colleges from 65-70 years.
- relaxation in the norms of setting up of Medical College in terms of requirement for land, faculty, staff, bed/bed strength and other infrastructure.
- Strengthening/upgradation of State Government Medical Colleges for starting new PG courses/Increase of PG seats.
- Establishment of New Medical Colleges by upgrading district/referral hospitals preferably in underserved districts of the country.
- Strengthening/ upgradation of existing State Government/Central Government Medical Colleges to increase MBBS seats.
- Strengthening of districts hospitals to run DNB/CPS courses.
Further, in order to encourage doctors to work in remote and difficult areas, the Medical Council of India, with the previous approval of Central Government, has amended the Post Graduate Medical Education Regulations, 2000 to provide:
- 50% reservation in Post Graduate Diploma Courses for Medical Officers in the Government service, who have served for at least three years in remote and difficult areas; and
- Incentive at the rate of 10% the marks obtained for each year in service in remote or difficult areas as upto the maximum of 30% of the marks obtained in the entrance test for admissions in Post Graduate Medical Courses.
The Minister of State (Health and Family Welfare), Sh Faggan Singh Kulaste stated this in a written reply in the Lok Sabha on July 28.
| PAEDIATRICIANS at CHCs | ||||||
| S. No. | State/UT | (As on 31st March, 2016) | ||||
| Required1 | Sanctioned | In Position | Vacant | Shortfall | ||
| [R] | [S] | [P] | [S-P] | [R-P] | ||
| 1 | Andhra Pradesh | 193 | 96 | 47 | 49 | 146 |
| 2 | Arunachal Pradesh | 63 | NA | 0 | NA | 63 |
| 3 | Assam | 151 | NA | 31 | NA | 120 |
| 4 | Bihar | 148 | NA | 8 | NA | 140 |
| 5 | Chhattisgarh | 155 | 155 | 15 | 140 | 140 |
| 6 | Goa | 4 | 0 | 2 | * | 2 |
| 7 | Gujarat | 322 | 62 | 44 | 18 | 278 |
| 8 | Haryana | 110 | 34 | 7 | 27 | 103 |
| 9 | Himachal Pradesh | 79 | NA | 2 | NA | 77 |
| 10 | Jammu & Kashmir | 84 | 61 | 44 | 17 | 40 |
| 11 | Jharkhand | 188 | 18 | 15 | 3 | 173 |
| 12 | Karnataka | 206 | 206 | 94 | 112 | 112 |
| 13 | Kerala | 225 | 14 | 17 | * | 208 |
| 14 | Madhya Pradesh | 334 | 334 | 76 | 258 | 258 |
| 15 | Maharashtra | 360 | 224 | 250 | * | 110 |
| 16 | Manipur | 17 | 2 | 2 | 0 | 15 |
| 17 | Meghalaya | 27 | NA | 0 | NA | 27 |
| 18 | Mizoram# | 9 | 0 | 0 | 0 | 9 |
| 19 | Nagaland | 21 | NA | 2 | NA | 19 |
| 20 | Odisha | 377 | 262 | 65 | 197 | 312 |
| 21 | Punjab | 150 | 145 | 32 | 113 | 118 |
| 22 | Rajasthan | 571 | 213 | 94 | 119 | 477 |
| 23 | Sikkim | 2 | NA | 0 | NA | 2 |
| 24 | Tamil Nadu | 385 | NA | 10 | NA | 375 |
| 25 | Telangana | 114 | 71 | 42 | 29 | 72 |
| 26 | Tripura | 20 | 0 | 0 | 0 | 20 |
| 27 | Uttarakhand | 59 | 54 | 14 | 40 | 45 |
| 28 | Uttar Pradesh | 773 | 523 | 154 | 369 | 619 |
| 29 | West Bengal | 349 | 287 | 22 | 265 | 327 |
| 30 | A& N Islands | 4 | 0 | 0 | 0 | 4 |
| 31 | Chandigarh## | 2 | NA | 3 | NA | * |
| 32 | D & N Haveli | 0 | 0 | 0 | 0 | 0 |
| 33 | Daman & Diu | 2 | 1 | 0 | 1 | 2 |
| 34 | Delhi | 0 | 0 | 0 | 0 | 0 |
| 35 | Lakshadweep | 3 | 0 | 0 | 0 | 3 |
| 36 | Puducherry | 3 | 4 | 3 | 1 | 0 |
| All India/ Total | 5510 | 2766 | 1095 | 1758 | 4416 | |
| Notes: | # Data for 2015 used | |||||
| ## Sanctioned data for 2013-14 used | ||||||
| NA: Not Available. | ||||||
| 1 | One per Community Health Centre | |||||
| All India figures for Vacancy and Shortfall are the totals of State-wise Vacancy and Shortfall ignoring surplus in some States / UTs | ||||||
| *: | Surplus. | |||||
| OBSTETRICIANS & GYNAECOLOGISTS at CHCs | ||||||
| S. No. | State/UT | (As on 31st March, 2016) | ||||
| Required1 | Sanctioned | In Position | Vacant | Shortfall | ||
| [R] | [S] | [P] | [S-P] | [R-P] | ||
| 1 | Andhra Pradesh | 193 | 96 | 55 | 41 | 138 |
| 2 | Arunachal Pradesh | 63 | NA | 3 | NA | 60 |
| 3 | Assam | 151 | NA | 55 | NA | 96 |
| 4 | Bihar | 148 | NA | 11 | NA | 137 |
| 5 | Chhattisgarh | 155 | 155 | 15 | 140 | 140 |
| 6 | Goa | 4 | 2 | 1 | 1 | 3 |
| 7 | Gujarat | 322 | 62 | 51 | 11 | 271 |
| 8 | Haryana | 110 | 31 | 6 | 25 | 104 |
| 9 | Himachal Pradesh | 79 | NA | 1 | NA | 78 |
| 10 | Jammu & Kashmir | 84 | 87 | 53 | 34 | 31 |
| 11 | Jharkhand | 188 | 31 | 39 | * | 149 |
| 12 | Karnataka | 206 | 206 | 170 | 36 | 36 |
| 13 | Kerala | 225 | 14 | 20 | * | 205 |
| 14 | Madhya Pradesh | 334 | 334 | 79 | 255 | 255 |
| 15 | Maharashtra | 360 | 244 | 119 | 125 | 241 |
| 16 | Manipur | 17 | 1 | 0 | 1 | 17 |
| 17 | Meghalaya## | 27 | 3 | 1 | 2 | 26 |
| 18 | Mizoram### | 9 | 0 | 0 | 0 | 9 |
| 19 | Nagaland | 21 | NA | 4 | NA | 17 |
| 20 | Odisha | 377 | 380 | 154 | 226 | 223 |
| 21 | Punjab | 150 | 150 | 70 | 80 | 80 |
| 22 | Rajasthan | 571 | 271 | 87 | 184 | 484 |
| 23 | Sikkim | 2 | NA | 0 | NA | 2 |
| 24 | Tamil Nadu## | 385 | 0 | 53 | * | 332 |
| 25 | Telangana | 114 | 71 | 63 | 8 | 51 |
| 26 | Tripura | 20 | 0 | 0 | 0 | 20 |
| 27 | Uttarakhand | 59 | 47 | 10 | 37 | 49 |
| 28 | Uttar Pradesh | 773 | 524 | 115 | 409 | 658 |
| 29 | West Bengal | 349 | 287 | 47 | 240 | 302 |
| 30 | A& N Islands | 4 | 3 | 0 | 3 | 4 |
| 31 | Chandigarh## | 2 | 5 | 9 | * | * |
| 32 | D & N Haveli | 0 | 0 | 0 | 0 | 0 |
| 33 | Daman & Diu | 2 | 1 | 0 | 1 | 2 |
| 34 | Delhi | 0 | 0 | 0 | 0 | 0 |
| 35 | Lakshadweep | 3 | 0 | 0 | 0 | 3 |
| 36 | Puducherry | 3 | 0 | 1 | * | 2 |
| All India/ Total | 5510 | 3005 | 1292 | 1859 | 4225 | |
| Notes: | ## Sanctioned data for 2015 used | |||||
| ### Data for 2015 used | ||||||
| All India figures for Vacancy and Shortfall are the totals of State-wise Vacancy and Shortfall ignoring surplus in some States / UTs | ||||||
| *: | Surplus | |||||
| 1 | One per Community Health Centre | |||||
| NA: Not Available. | ||||||









